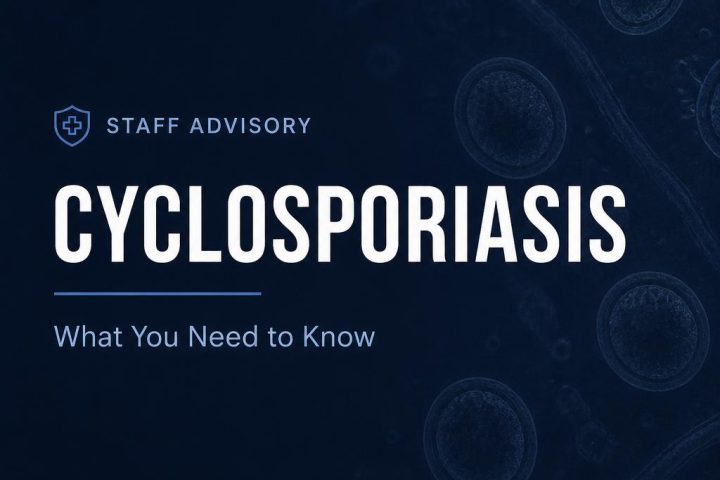
| “L858R” mutated EGFR gene and resulting protein T>G transversion at position 2573 in Exon 21 resulting in replacement of leucine (L) with arginine (R) |
|||||||||||||||||||||||
| T | T | T | G | G | G | C | G | G | G | C | C | A | A | A | C | T | G | C | T | G | G | G | T |
| 25 66 |
25 67 |
25 68 |
25 69 |
25 70 |
25 71 |
25 72 |
25 73 |
25 74 |
25 75 |
25 76 |
25 77 |
25 78 |
25 79 |
25 80 |
25 81 |
25 82 |
25 83 |
25 84 |
25 85 |
25 86 |
25 87 |
25 88 |
25 89 |
| F | G | R | A | K | L | L | G | ||||||||||||||||
| 856 | 857 | 858 | 859 | 860 | 861 | 862 | 863 | ||||||||||||||||
BLUF Statement (bottom line up front):
Cigarette smoking is the cause of most lung cancers which occur in both men and women. About 4% of male lung cancers and 19% of female lung cancers occur in never smokers or in long-term ex-smokers. Adenocarcinoma is the most common kind of lung cancer which occurs in non-smokers. In multiple cases, asbestos plaintiff attorneys have argued that non-smokers developed lung cancer because of asbestos exposure, whether or not asbestosis (or an equivalent fiber burden) was present. Advances in DNA mutation analysis provide a better explanation. Mutations in the epidermal growth factor receptor (EGFR) gene situated on human chromosome 7 are an important cause of lung cancer in non-smokers. Asbestos exposure does not cause EGFR mutation.
Epidemiology
In 2015 there were a total of 2,712,630 deaths reported in the United States. Heart disease was the cause of 633,842 or 23.4% of all deaths in the U.S. while cancer of all types caused 595,930 or 22.0%. Significantly more men died of cancer than did women with a ratio of 1.4:1. In both men and women, lung cancer was by far the most important cause of cancer death in the U.S., causing 86,380 deaths in men (28% of male cancer deaths) and 71,660 deaths in women (26% of female cancer deaths) compared to, for example, 28,094 prostate cancer deaths (9% of male cancer deaths) and 41,592 breast cancer deaths (15% of female cancer deaths).
There are 2 main kinds of lung cancer: non-small cell lung cancer, which includes squamous cell lung cancer, pulmonary adenocarcinoma and large cell lung cancer, and small cell lung cancer. Approximately 50% of all lung cancers are adenocarcinomas, about 25% of lung cancers are squamous cell and 15% are small cell. Large cell lung cancer and other less common types of lung cancer make up the rest.
Almost 100% of squamous cell and small cell lung cancers occur in current or former cigarette smokers. In men, about 4% of pulmonary adenocarcinomas occur in non-smokers [1] [2] whereas 19% of women who suffer from pulmonary adenocarcinoma are non-smokers or long-term ex-smokers. [3]
The age-adjusted incidence rate (AAIR) of lung cancer in female never smokers 40 to 79 years old has been reported to be 14 to 20 per 100,000 person-years.[4] In contrast, the AAIR in current smokers is 12 to 30 times higher. Approximately 70% of lung cancers which occur in female never smokers are adenocarcinomas.
Asbestos exposure and lung cancer
Almost all lung cancers which occur in former asbestos workers occur in current or ex-smokers. It is my opinion that asbestos exposure increases the risk of lung cancer, but only in those workers who have pulmonary parenchymal asbestosis or an equivalent asbestos fiber burden in lung tissue. Although strongly supported by the peer-reviewed published medical literature, this opinion is not universally accepted and disagreement about the need to demonstrate asbestosis or an equivalent fiber burden in order to establish causation is at the crux of many asbestos litigation cases.
In multiple cases, asbestos plaintiff attorneys have argued that lung cancer patients who were never smokers or who have a history of long-term smoking cessation developed their cancer because of asbestos exposure, whether or not asbestosis (or an equivalent fiber burden) was present and whether or not the plaintiff’s history of asbestos exposure was substantial. Simply stated, the argument has been that “something” must have caused the patient’s lung cancer and that asbestos exposure, no matter how minimal, must have been the something.
Advances in DNA mutation analysis have revealed the etiology of many cases of lung cancer in never smokers and long-term ex-smokers.
The genetic code
The nuclei of human cells contain 23 pairs of chromosomes. Each chromosome is composed of a large double-stranded helical molecule named deoxyribonucleic acid (DNA) and protein. DNA encodes the genetic instructions for the production of all the proteins needed for the construction and function of the organism. Genes are hereditary units composed of a length of a chromosome which encode for specific proteins. In total, there are approximately 20,000 human genes.
With the exception of mature red blood cells, all human cells contain chromosomes and the entire genetic code. DNA and the genetic code are often incorrectly referred to as providing a “blueprint” for cellular production. A blueprint for a building includes a schematic representation of every single physical structure in the building while in contrast, a recipe for a cake contains a list and quantity of ingredients and instructions about how and in what sequence the ingredients are to be combined. When heated to the proper temperature, the mixture of ingredients specified by the recipe invariably produces a cake. Although each cake produced is very similar to all other cakes, it is unique and certainly, the recipe does not include a physical representation of each and every cake crumb. Thus, the genetic code is much more like a cake recipe than like a building blueprint.
A mutation is an error in the DNA code, that is, an error in the recipe. Genes undergo mutation when their DNA sequence changes.
“Germline” refers to cells which make up eggs and sperm; thus, a germline mutation is a DNA alteration inherited from a person’s mother and/or father. “Somatic” means “of the body”. A somatic mutation is a DNA alteration that occurs only in a particular person’s body cells, for example, a mutation in a single bronchial cell which then divides uncontrollably to form a lung cancer. Germline and somatic mutations are both “genetic” because they are alterations in genetic material, i.e. DNA, but only germline mutations are “inherited”.
Different mutations can have very different consequences. Some mutations result in the production of proteins which are so aberrant that the altered cell promptly dies, whereas other mutations result in disease only after many years. Some mutations are beneficial and provide the organism with a survival advantage over its fellow creatures which do not carry such mutated genes. Such mutations are the basis of evolutionary change.
Some mutations, individually or in combination, cause critical changes in one or more cellular characteristics which collectively are recognized as “cancer”. Cell characteristics of cancers include:
- Self-sufficiency in growth signals
- Limitless replicative potential
- Insensitivity to growth-inhibitory signals
- Evasion of apoptosis – resistant to programmed cell death
- Sustained angiogenesis: tumors stimulate the growth of their own blood supply
- Ability to invade and metastasize: typically the cause of cancer death
EGFR mutations
The membranes of normal cells contain epidermal growth factor receptors, the production of which is controlled by the function of the EGFR gene which is situated on the short (p) arm of human chromosome 7. In the normal cell, EGFR is responsive to epidermal growth factors and helps to control cell proliferation and other essential cell functions. Different kinds of mutation in the EGFR gene result in constitutive activation of signal transduction pathways (a protein switch stuck in the “on” position), leading to uncontrolled cell proliferation, i.e. cancer.
In 40% to 50% of pulmonary adenocarcinomas which occur in never smokers and long-term ex-smokers there is a mutation of the epidermal growth factor receptor (EGFR) gene. In pulmonary adenocarcinomas which harbor EGFR gene mutations, the mutations are the cause and the mechanism of the lung cancer.
To date, the initiator or initiators, if any, of EGFR mutations have not been identified and the most likely cause of EGFR mutation is spontaneous error in DNA replication (almost 2/3 of cancer-inducing mutations are somatic mutations which result from spontaneous errors of DNA replication [5]). Because of the observed epidemiological pattern, that is, the fact that EGFR mutation lung cancers occur much more commonly in never-smokers than in smokers and the fact that they often occur in women, including young women, there is no reason to believe or anticipate that EGFR mutation has anything to do with asbestos exposure. To date, four reports have been published in the peer-reviewed published medical literature which deal with EGFR mutation in asbestos-exposed individuals. None have demonstrated a cause and effect relationship between asbestos exposure and EGFR mutation.
In 2017, Paris et al [6] published an analysis of the BioCAST/IFCT-1002 cohort which consisted of 384 never smokers who had lung cancer and who were evaluated at one of 75 participating medical centers in France. The BioCast cohort, sponsored by the French Collaborative Intergroup for Thoracic Cancer Research, was the “largest and most comprehensive LCINS [lung cancer in never smokers] analysis in a European population.” [7] Paris et al demonstrated that asbestos-exposed never smokers who had lung cancer “displayed a significantly lower rate of EGFR mutations (20% versus 44%, p=0.033)” and concluded, “asbestos-exposed patients have a lower chance of EGFR mutations.”
Routine EGFR mutation testing and treatment
Patients whose pulmonary adenocarcinomas harbor certain types of EGFR mutation often experience dramatic therapeutic response to a new class of anti-tumor drugs named tyrosine kinase inhibitors (TKI’s) including first-generation TKI (erlotinib, brand Tarceva) or second generation TKI (afatinib). TKI’s specifically target a cleft in the structure of mutated EGFR, the critical genetic lesion that promotes proliferative signals in cancer cells. Therapeutic responses to TKI’s may include resolution or near-resolution of pulmonary parenchymal masses and even resolution of metastatic foci; however, after 9 to 13 months patients who experience good initial response commonly suffer from reactivation and metastatic spread of their cancer caused by the acquisition by the cancer of an additional mutation. In 2015 reports of successful treatment of such patients was described using third generation TKI’s Osimertinib and Rociletinib.
It is now routine to test newly detected pulmonary adenocarcinomas, especially those which occur in female non-smokers, for EGFR mutation. The medical records of such patients will usually include the results of testing for EGFR and other lung cancer mutations.
Bibliography
[1]. McDuffie HH; Klaassen DJ; Dosman JA: Determinants of cell type in patients with cancer of the lungs. Chest 1990 Nov;98(5):1187-93. [2]. Barbone F, Bovenzi M, Cavallieri F, Stanta G: Cigarette smoking and histologic type of lung cancer in men. Chest 1997 Dec;112(6):1474-9. [3]. Radzikowska E, Glaz P, Roszkowski K. Lung cancer in women: age, smoking, histology, performance status, stage, initial treatment and survival. Population-based study of 20 561 cases. Ann Oncol. 2002 Jul;13(7):1087-93. [4]. Wakelee HA, Chang ET, Gomez SL, Keegan TH, Feskanich D, Clarke CA, Holmberg L, Yong LC, Kolonel LN, Gould MK, West DW. Lung cancer incidence in never smokers. J Clin Oncol. 2007 Feb 10;25(5):472-8. [5]. Tomasetti C, Li L, Vogelstein B. Stem cell divisions, somatic mutations, cancer etiology, and cancer prevention. Science. 2017 Mar 24;355(6331):1330-1334. [6]. Paris C, Do P, Mastroianni B, Dixmier A, Dumont P, Pichon E, Chouaid C, Coudert B, Foucher P, Fraboulet S, Locatelli-Sanchez M, Baize N, Dansin E, Moreau L, Vincent M, Missy P, Morin F, Moro-Sibilot D, Couraud S; BioCAST/IFCT-1002 study investigators; to the BioCAST/IFCT- 1002 study. Association between lung cancer somatic mutations and occupational exposure in never-smokers. Eur Respir J. 2017 Oct 26;50(4). [7]. Couraud S, Souquet PJ, Paris C, Dô P, Doubre H, Pichon E, Dixmier A, Monnet I, Etienne-Mastroianni B, Vincent M, Trédaniel J, Perrichon M, Foucher P, Coudert B, Moro-Sibilot D, Dansin E, Labonne S, Missy P, Morin F, Blanché H, Zalcman G; French Cooperative Intergroup IFCT. BioCAST/IFCT-1002: epidemiological and molecular features of lung cancer in never-smokers. Eur Respir J. 2015 May;45(5):1403-14.